Retinal Detachment
What is a retinal detachment?
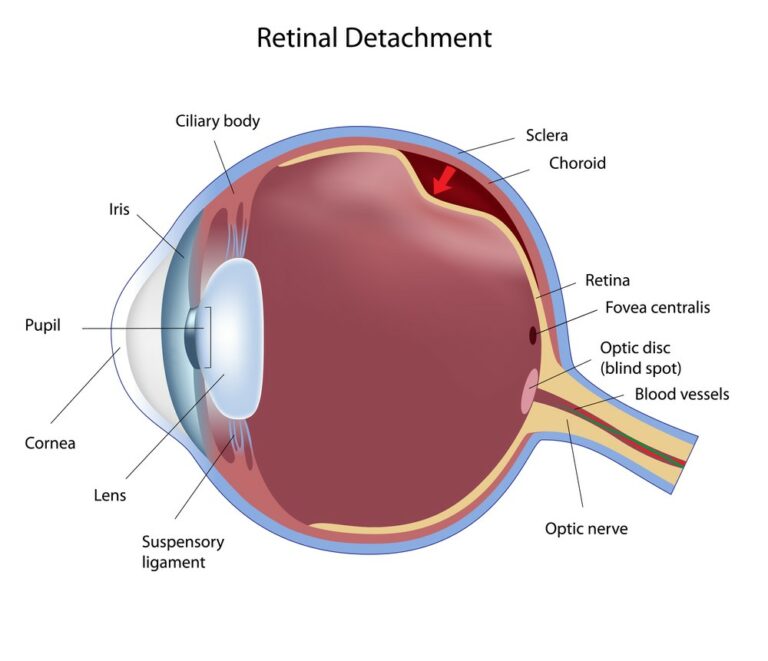
A retinal detachment is a serious eye condition that occurs when the retina (the layer of tissue with light-sensitive cells lining the back of your eye) separates from the other layers and underlying structures at the back of your eye (such as the retinal pigment epithelium, the layer of pigmented cells at the retina), which may cause blindness. Some of its common symptoms include; flashes of light, blurred vision, and the presence of floaters.
This overview will cover how common is retinal detachment, its causes, who are at risk, its symptoms, how it is detected, the available treatment options, as well as the possible prevention methods.
How common is retinal detachment?
Retinal detachments affect about 1 in 10,000 people in the world. Ethnic variations exist and it is well known that a patient of Chinese origin is 3 times more likely to need retinal detachment surgery compared to their Indian counterparts. There are reports that some developing countries have a lower rate of new cases of the condition; however, due to poor access to facilities and delayed detection and management of the condition, the risk of blindness is higher in this group of people.
How do you get a detached retina?
The vitreous or vitreous humour contains a jelly-like substance that permeates the middle of your eye. As you age, the volume of the vitreous in your eyes will progressively decrease. Posterior vitreous detachment (PVD) can develop when the gel in the vitreous humour separates from the retina.
In a normal eye, movement can cause the vitreous to move around the retina without much concern. However, sometimes the vitreous may stick to the retina and pull at it firmly enough to tear it. Once the retina is torn, fluid can seep through the tear and detach the retina.
What are the types & causes of retinal detachment?
There are three different types of retinal detachment that can occur via 3 mechanisms:
- Rhegmatogenous:
Rhegmatogenous retinal detachment is the most common type of retinal detachment and is attributable to ageing. As you age, thinning of the vitreous humour in your eye would move around the retina when your eye moves and latch onto the retina and pull it. The resultant tear in your retina permits fluid to pass through and accumulate underneath the retina. Consequently, such fluid pulls the retina away from underlying tissues and the retinal cells are separated from the layer of blood vessels that provides oxygen and nourishment. The affected areas where the retina detaches lose their blood supply and stop working. If this type of detachment is left untreated, it can progress rapidly and lead to blindness
- Tractional:
The second type of retinal detachment is a tractional retinal detachment as a result of other underlying health conditions such as diabetes. This type of retinal detachment happens when bands of scar tissue develop on the surface of the retina, prompting the retina to pull away from the back of the eye.
- Exudative or Serous:
Exudative (or serous) retinal detachment is the third type of retinal detachment whereby fluid accumulates underneath the retina without any consequent holes or tears in the retina itself. This type of retinal detachment is usually caused by eye injuries or tumors and does not always necessitate surgery
Who is at risk of retinal detachments?
Generally, the older you get, the higher the risk of you getting a retinal detachment, especially if you are over the age of 50 years. Also, if you have previously suffered a retinal detachment in one eye, you would be more vulnerable to developing the condition in the other eye.
Retinal detachment can be hereditary, so if you have a family history of retinal detachment, you may be at a greater risk. You may also be more susceptible to getting the condition if you suffer from high myopia (nearsightedness) or had prior eye surgery such as cataract removal.
The risk factors for a retinal detachment can be divided into those that are associated with patient (lifestyle) factors and anatomical (due to other eye conditions) factors.
Patient/lifestyle factors include:
- Increasing age
- Trauma
- Previous retinal detachment
- Previous intraocular surgery
- Family history
Factors due to other eye conditions include:
- Myopia (short-sightedness)
- Retinal tears
- Lattice degeneration (areas of thinned retina)
Of these, myopia, lattice degeneration, and increasing age are most strongly associated with retinal detachments. Patients can find out if they are at risk due to other eye conditions by booking an appointment with a local optometrist for a dilated retinal examination.
What are the symptoms of a retinal detachment?
- Experiencing flashing lights (or ‘seeing stars’) abruptly
- Experiencing blurry vision
- Perceiving many new floaters (that look like small dots, circles, cobwebs, lines and specks) in your field of vision
- Noticing a shadow surfacing in your peripheral (side) vision
- Noticing a gray curtain enveloping part of your field of vision
The classic symptoms of a retinal detachment are new-onset (development) floaters, flashes, as well as possibly a curtain-like shadow in the peripheral (outer) vision. If the macula (part of the retina at the back of the eye responsible for central vision) is involved, then the central vision will be perceived as blurred. Rarely, a retinal detachment may exist for a long time in the eye but the patient may not show any symptoms.
As a detached retina would pose a major threat to your vision, it is important to consult with your eye doctor immediately once you display symptoms of this eye condition. The longer you delay the treatment of retinal detachment, the greater your risk of permanent vision loss in the affected eye.
If you experience any of these signs and symptoms, schedule an appointment with an eye health professional to get your eyes checked. It is also important to note that the development of eye conditions may even start before symptoms appear, which makes going for regular and timely eye checks that much more essential.
How is a retinal detachment detected?
A retinal detachment is detected by using a special lens and a slit lamp to examine the retina. The patient has mydriatic (dilating) drops instilled to expand the pupil, which subsequently facilitates visualisation of the retina. Special contact lenses and ancillary equipment called an indenter may be used to bring the peripheral retina into view for the examiner to aid in identifying a break in the retina.

What are the treatment options for a retinal detachment?
Retinal detachments, particularly those of a rhegmatogenous nature, require urgent treatment. If the macula is involved, treatment ideally should be performed within 24 to 72 hours upon diagnosis. If the macula is not involved, then treatment may be performed within 7 to 10 days upon diagnosis as earlier treatment has not been shown to improve visual outcomes.
The goal of repair in a rhegmatogenous detachment is to identify the break and treat it. Treatment options depend on patient factors and the nature of the detachment. Several options available to treat the condition are:
- Pars plana vitrectomy
- Pneumatic retinopexy
- Scleral buckle
Pars plana vitrectomy
This type of surgery is used to address more complicated conditions of retinal detachments. This procedure involves the insertion of ports to access the internal cavity of the eye. The vitreous is removed using specialised instruments and a thorough search is performed to find the retinal break. Subretinal fluid is removed from the retina and a tamponade such as gas or oil is inserted to keep the retina placed and fixed in close proximity.
Pneumatic retinopexy
Some patients may be suitable candidates for this procedure, which involves the injection of a gas bubble into the eye. The criteria for treatment with pneumatic retinopexy varies but are suited when there is a good view to the retina, a single break in a superior position, and the patient is able to position their head as required by the surgeon. In some centres, this procedure can be performed in an outpatient, rather than an operation theatre, setting.
Scleral buckle
A scleral buckle is a silicone band that is inserted around the eye and is positioned underneath the extraocular muscles. The buckle relieves the traction and flattens the retina and an adjunctive cryotherapy or laser is often administered [5].
Treatment of tractional retinal detachments follows similar principles as treating rhegmatogenous detachments with the aim being to relieve tractional bands via pars plana vitrectomy. Adjunctive scleral buckles may also be used. Serous retinal detachments are not treated surgically and its treatment is aimed at addressing the underlying issue such as inflammation.
Is it possible to prevent retinal detachments?
Most retinal detachments occur without any clear and sudden cause but those at higher risk such as patients with myopia, may consider the use of protective eyewear when undergoing contact sports.
Once you have been diagnosed as being at risk for a retinal detachment, you may wish to avoid activities involving a certain amount of risk of pressure to the eyes such as hang-gliding or bungee jumping.
Ultimately, if detected and treated early and patients only present themselves with new symptoms (floaters and flashes), it is possible that the tear can be treated with laser retinopexy before it progresses into a retinal detachment.
The reality is that there is no way to completely prevent retinal detachment. Hence, regular eye check ups are important to detect potential eye health problems early on. Consult an eye health professional immediately once you detect any signs of a retinal detachment, especially in the early stages. Prompt treatment can mitigate the risk of permanent vision loss as a result of an untreated retinal detachment.
DISCLAIMER: THIS WEBSITE DOES NOT PROVIDE MEDICAL ADVICE
The information, including but not limited to, text, graphics, images and other material contained on this website are for informational purposes only. No material on this site is intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen, and never disregard professional medical advice or delay in seeking it because of something you have read on this website.
References
- D. A. Brinton and C. P. Wilkinson, “Pathogenesis, Epidemiology, and Natural Course of Retinal Detachment,” Retinal Detachment. 2009. doi: 10.1093/oso/9780195330823.003.0006.
- D. Yorston and S. Jalali, “Retinal detachment in developing countries,” Eye, vol. 16, no. 4. pp. 353–358, 2002. doi: 10.1038/sj.eye.6700188.
- D. Mitry, D. G. Charteris, B. W. Fleck, H. Campbell, and J. Singh, “The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations,” Br. J. Ophthalmol., vol. 94, no. 6, pp. 678–684, Jun. 2010.
- R. Scott and G. Kirkby, “Treatment of macula-on retinal detachments,” Eye, vol. 21, no. 7. pp. 1008–1008, 2007. doi: 10.1038/sj.eye.6702810.
- A. J. Brucker and T. B. Hopkins, “Retinal detachment surgery: the latest in current management,” Retina, vol. 26, no. 6 Suppl, pp. S28–33, Jul. 2006.
Tools Designed for Healthier Eyes
Explore our specifically designed products and services backed by eye health professionals to help keep your children safe online and their eyes healthy.